The NHS is the largest employer in the UK with more than 1.4 million employees. Its workforce is under growing pressure. The population is ageing, increasing demand on healthcare services. The number of staff vacancies are high. The Health Foundation has predicted a shortfall of nearly 1 in 10 (9%) of all NHS workforce posts by 2030 - 2031.
The Department of Health and Social Care has made support for the workforce a key research priority. It is aiming to develop and evaluate technology-assisted workforce solutions both to reduce the burden on staff and to improve patient outcomes. Increased use of technology in healthcare is central to the NHS Long term Plan.
This Collection highlights examples of recent NIHR research that demonstrate ways in which digital technology can improve care while reducing the demands on staff. The technologies include computer decision aids, remote patient monitoring, online support for patients and staff, and virtual reality in psychological therapies.
The research shows that these technologies could bring multiple benefits, both to the workforce, and to patients. They could save healthcare professionals’ time, increase the number of people a skilled professional can support, and enable more sustainable workforce models. At the same time, they can promote safer and more personalised care.
The Collection provides useful information for those commissioning and delivering services, including people working across integrated care systems. It sits alongside 2 other Collections: One collection helps members of the public understand digital health technology, and the other describes promising examples of artificial intelligence, or AI, for healthcare.
Computer decision aids
Computer decision aids can quickly and accurately rule out heart attacks in A&E
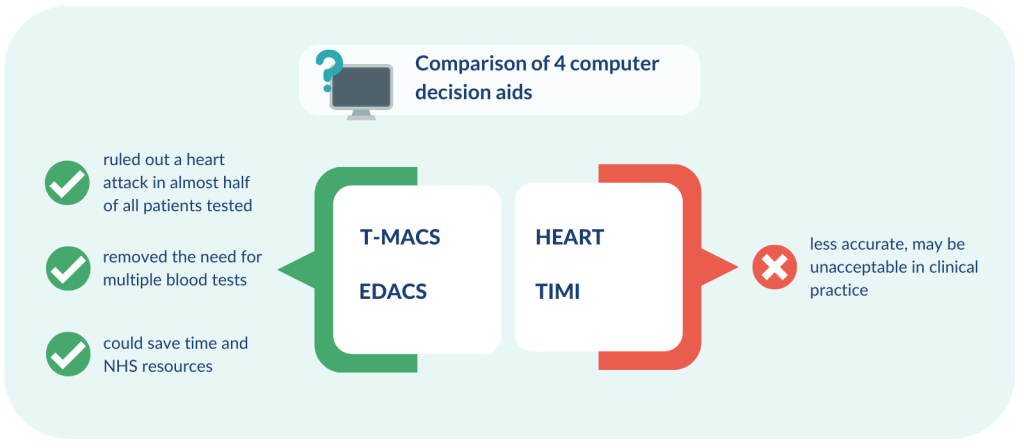
Most people (around 9 out of 10) who attend A&E with chest pain have not had the heart attack they feared. Computer decision aids can help doctors accurately rule out heart attacks. The decision aids combine the results of a single blood test with information on the patient’s symptoms, previous medical history and findings from physical examinations. Several decision aids exist, so research directly compared the diagnostic accuracy of 4 different types.
The study involved 999 people arriving at A&E departments in England. All had a blood test on arrival. It found that the Troponin-only Manchester Acute Coronary Syndromes (T-MACS) and the Emergency Department Assessment of Chest Pain (EDACS) decision aids were the most accurate. They ruled out a heart attack in almost half of all patients tested, removing the need for multiple blood tests. This could save staff time and NHS resources, and either identify the need to act urgently, or allow staff to provide reassurance. The remaining patients needed a second blood test for cardiac markers.
The other 2 decision aids tested in the study, History, ECG, Age, Risk factors and Troponin (HEART) and Thrombolysis in Myocardial Infarction (TIMI) were less accurate than T-MACS and EDACS and may be unacceptable for use in clinical practice. T-MACS has been implemented at Manchester Royal Infirmary.
Computer decision aids support safe prescribing
Two computer-based interventions, which aim to improve prescribing safety in primary care, have been rolled out across England over the past few years. The first system (computerised decision support, or CDS) raises a warning when a clinician is about to prescribe a medicine that could increase a patient’s risk of harm.
The second method (PINCER), led by pharmacists, searches people’s medical notes for errors that have already happened. Pharmacists, GPs and other clinicians work together to address them.
Researchers explored how to ensure that the interventions have a long-term impact, beyond the initial roll-out phase. They examined 48 documents, interviewed 27 relevant professionals and carried out 2 workshops which also involved members of the public.
The team identified 5 strategies to increase the long-term success of the interventions.
- Ensure a good fit with current practice and priorities through ease of use and integration into IT systems
- Engage hearts and minds through leadership and alignment with professional values
- Build resilience with a team approach which involves all staff members
- Align prescribing safety guidelines with secondary care through shared IT infrastructure and communication
- Consider using PINCER and CDS together; share data for best practice
“Our study provides teams working across integrated care systems with evidence-based considerations for how they might introduce and sustain the impact of PINCER and computerised decision support in primary care.”
Richard Keers, Senior Clinical Lecturer in Pharmacy, University of Manchester
The strategies form the basis of a toolkit to help local managers and clinicians make best use of these interventions. They can choose the strategies that fit their local situation.
Electronic monitoring
A sensor under the skin improves blood sugar levels in preterm infants
High blood sugar, low blood sugar or unstable blood sugar (glucose) levels are common in premature infants, especially those born extremely preterm (before 28 weeks of pregnancy). They are linked to developmental problems during childhood, and an increased risk of long-term health conditions.
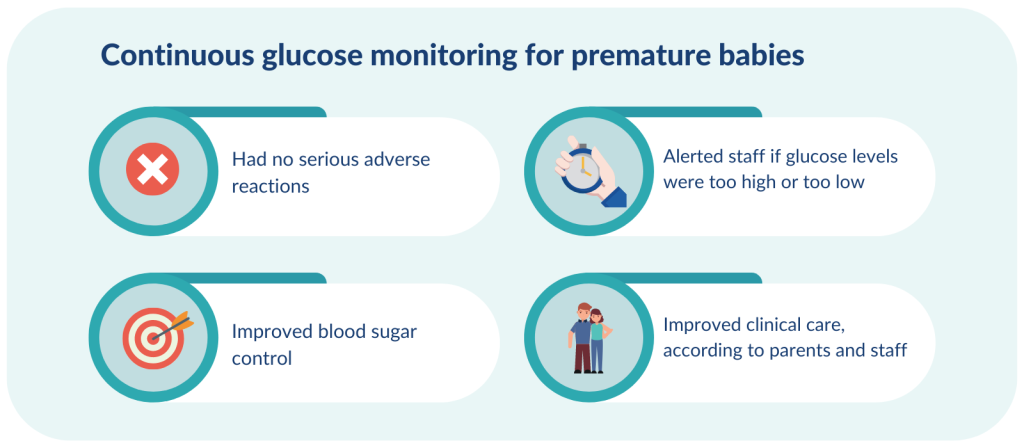
Keeping premature infants’ blood sugar at a constant level is challenging. Standard intensive care means staff taking blood samples every few hours to test glucose levels; even this cannot always protect infants against extreme blood sugar levels. Recent research compared continuous glucose monitoring (CGM), through an electronic sensor under the skin, with standard care. The sensor automatically alerts healthcare professionals when glucose levels are too high or too low.
The study analysed data on 155 premature infants, who all had a CGM sensor inserted. Staff received readings from 70 of the infants; the others received standard care.
CGM was more effective at keeping blood sugar levels within the target range compared to standard care. Staff could alter treatment quickly and avoid dramatic swings in sugar levels. This could improve infants’ long-term health.No infant had a serious adverse reaction to the CGM device and most parents and staff felt that CGM improved clinical care. The neonatal unit in Cambridge has made CGM standard practice for extremely preterm infants.
“The use of CGM is well-established in children with diabetes. It allows earlier detection and prevents exposure to extreme swings in blood glucose. Using CGM more widely could allow us to better manage the blood glucose concentrations of babies and children. It could reduce the risk of death and of long-term health conditions.”
May Ng, Consultant Paediatric Endocrinologist, Southport and Ormskirk Hospital NHS
Home monitoring improves blood pressure control
High blood pressure increases a person’s risk of heart disease and strokes; the risk can be reduced by lowering blood pressure. Researchers investigated whether a digital intervention could help. The intervention helped people monitor their blood pressure at home and prompted GPs to change their medication when blood pressure was raised over time. It included optional lifestyle advice and motivational support.
The trial involved 622 people; all were taking blood pressure medication but their blood pressure was still poorly controlled. Half the participants received the digital intervention, the others received usual care.
After 1 year, people using the intervention had better controlled (lower) blood pressure than people receiving usual care. GPs were more likely to adjust people’s blood pressure medication, which suggests the intervention led to optimised treatment.
This digital intervention is likely to represent value for money for the NHS and could be implemented at scale in a cost-effective way. The researchers say the reduction in blood pressure seen in the trial could be expected to reduce the number of people having a stroke by 10-15%. Future studies will be needed to check that these predicted benefits are achieved in practice. The intervention could also be developed further, to ensure that it can be used by older people and those from disadvantaged backgrounds.
Online support for staff
Remote, real-time intervention supports a more sustainable workforce model
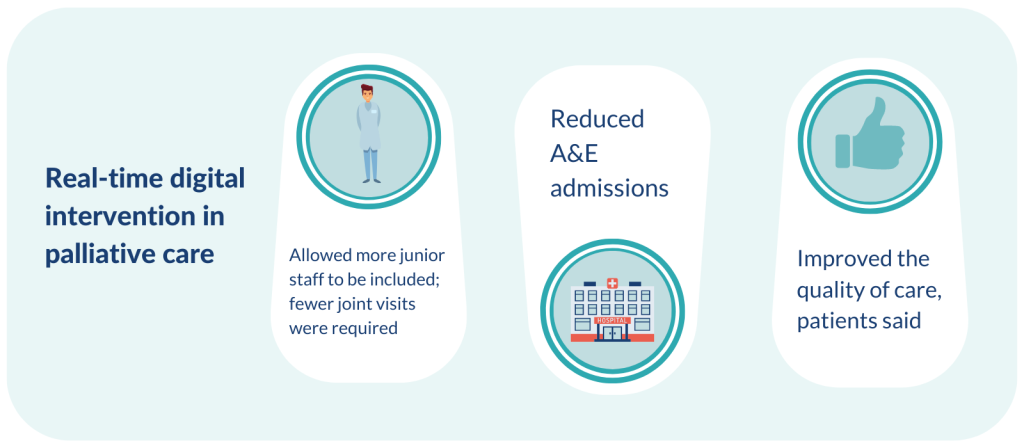
Community palliative and end of life care services rely on highly trained healthcare professionals to enable them to make decisions about care. This means care may be costly, inflexible, difficult to scale and inefficient. Digital technology could help. One intervention was designed to enable senior staff to provide remote, real-time support, and to delegate tasks to more junior colleagues.
Researchers evaluated the real-world implementation of the intervention in one specialist community palliative care service in Sheffield. They considered the seniority of staff attending community hospice service visits and whether staff attended alone, hospital use by patients, and patients’ views on the quality of their care. Findings were compared before and after the intervention was implemented.
The digital intervention allowed the service to include more junior staff and fewer joint visits to patients were needed. This suggests a more sustainable model of care. A&E admissions were reduced and patients felt the quality of care improved. The researchers say their study demonstrates that digital technology can support service redesign and help address the healthcare workforce crisis, while improving key outcomes such as patient experience. The redesigned service continues to be used in Sheffield.
Online support for patients
Online treatment for children with tics is effective and requires less therapist time
Up to 1 in 100 schoolchildren have tic disorders, such as Tourette’s Syndrome. Tics are sudden, rapid movements or sounds that are difficult to control. They can be distressing and disrupt a young person’s school and social life. Face-to-face behaviour therapy is recommended, but access is limited by the lack of trained specialists and uneven distribution of services across the country.
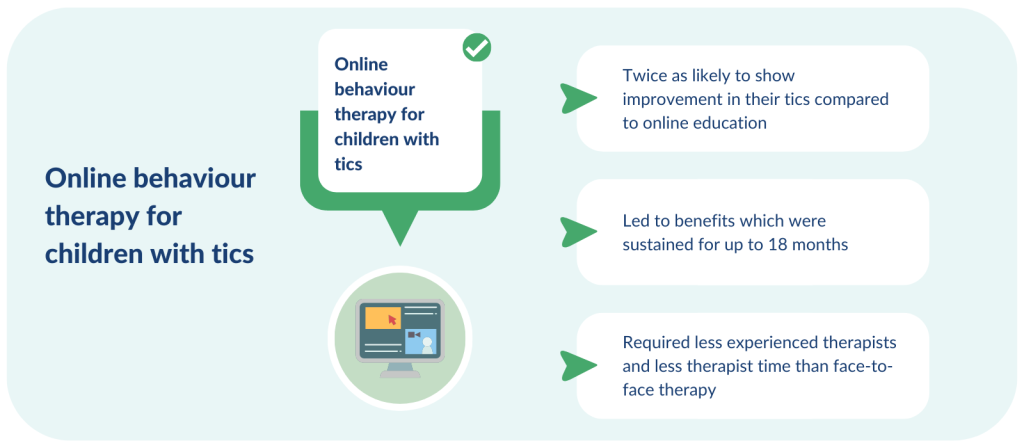
Recent research investigated online behaviour therapy (in which children are helped to suppress their tics while tolerating the urge to tic), supported by therapists and parents, and whether this could be an effective option.
The trial involved 224 children, aged 9 to 17 years, with a moderate or severe tic disorder. It compared this online behaviour therapy to an online package of education. All participants had access to a therapist via online messaging.
Overall, children who received online behaviour therapy were twice as likely to show improvement in their tics than those who received online education. Benefits were sustained for up to 18 months after the start of treatment. The treatment was likely to be value for money.
The new online treatment could be delivered by less experienced therapists, and it required less therapist time than traditional face-to-face therapy. This could greatly increase the availability of a lasting and cost-effective behavioural treatment, the researchers say.
“Access to evidence-based behavioural treatments for both children and adults with tics is unacceptably limited; many more could benefit. Advances in methods of delivering therapy that may improve provision is therefore important. Tourettes Action supports all developments to address this unmet need.”
Jeremy Stern, Honorary Medical Advisor and Trustee, Tourettes Action
Self-management website improves eczema symptoms in children and young people
Self-management can empower people with long-term conditions to take in control of their treatment. It can improve outcomes and reduce the number of doctors’ appointments needed.
About 1 in 5 children and 1 in 10 adults in the UK have eczema. They may have dry, itchy, cracked and sore skin which affects their quality of life.
People with eczema say they receive insufficient or conflicting information about their condition. Recent research therefore investigated whether access to an evidence-based website to support self-management of eczema (EczemaCareOnline) offered benefits over standard advice. One version of the website is aimed at parents and carers of children with eczema; another is for young people starting to self-manage their eczema.
Two trials were conducted. The first included 340 parents and carers of children (0 – 12 years) with eczema; the second, 337 young people (13 – 25 years) with eczema. In both trials, half the participants had access to the new website.
“The conclusion that young people and parents became more confident in managing their eczema is particularly significant. Carers often tell us that this confidence helps them to advocate for the needs of their children at nursery/school and to access any additional support their child may need, such as with their mental health.”
Suzi Holland, Deputy Chief Executive Officer, Eczema Outreach Support
Both trials found access to the website led to greater improvements in eczema symptoms after 6 months compared to standard care. Improvements were small but significant, and sustained at 1 year. The researchers say the websites increased the confidence of parents and young people in managing eczema.
The website is free to use without registration. The researchers hope healthcare professionals will encourage carers and young people to use it. They say the small improvement in symptoms is valuable, given the low cost and high scalability of the online support, and absence of identifiable harms.
Use of virtual reality
Therapy delivered by virtual reality helps people with psychosis overcome fear of leaving home

People with psychosis may experience such intense fears about being outside that they avoid leaving home altogether. This greatly affects their relationships and daily activities. New research investigated whether virtual reality could be an effective way to deliver therapy. The virtual therapy allowed people to practise everyday situations such as leaving home, being in a cafe, shop, doctor's surgery, pub, and getting on a bus.
The trial involved 346 people with psychosis. Half received usual care, the others received virtual reality therapy. They were guided through simulations by a virtual therapist. A variety of mental health staff, including peer support workers, provided support.
Virtual reality therapy reduced people’s avoidance of, and distress in everyday situations. It was especially effective for those with severe difficulties, such as not being able to leave home unaccompanied, among whom the benefits lasted for 6 months. The therapy is built into virtual reality headsets which are easy to use, and support can be provided by non-specialists. This means the therapy could be delivered on a large scale in clinical services, the researchers say.
Conclusion
The 8 recent examples of research in this Collection highlight just a few ways technology could help healthcare professionals to deliver high-quality care.:
- Computer decision aids enabled rapid and safe clinical and treatment decisions.
- Electronic monitoring improved care and reduced pressure on staff.
- Online support for staff enabled specialists to work with more junior colleagues while improving the experience for patients.
- Online support for patients improved access to care and patients’ capacity to manage their own condition; this in turn could reduce the pressure on staff in hospital and primary care.
- Virtual reality enabled non-specialists to support the delivery of specialist mental health support, reducing the pressure on specialist staff.
Supporting the health and care workforce is a key area of research interest for the Government and the NIHR. Technology-assisted workforce solutions which reduce the burden on staff while maintaining patient outcomes, are a priority. The aim is to find and implement effective and efficient ways of delivering care that meet the needs of the population.
Author: Jemma Kwint, Senior Research Fellow, NIHR Evidence
How to cite this Collection: NIHR Evidence; Digital technology in the NHS: reducing staff pressures, improving care; June 2023; doi: 10.3310/nihrevidence_58798
Disclaimer: This Collection is based on research which is funded or supported by the NIHR. It is not a substitute for professional healthcare advice. Please note that views expressed are those of the author(s) and reviewer(s) at the time of publication. They do not necessarily reflect the views of the NHS, the NIHR or the Department of Health and Social Care.
NIHR Evidence is covered by the creative commons, CC-BY licence. Written content and infographics may be freely reproduced provided that suitable acknowledgement is made. Note, this licence excludes comments and images made by third parties, audiovisual content, and linked content on other websites.